
ABSTRACT:
Background: It is well known that quality of life is an integral part in the outcome evaluation process of psoriasis treatment. Very few studies, however, examined the effect of climatotherapy at the Dead Sea on quality of life of such chronically ill patients.
Objectives: To determine the effect of the Dead Sea climatotherapy on the quality of life of patients with psoriasis vulgaris and psoriatic arthritis.
Methods: A total of 119 patients participated in an observational prospective study carried out at the Deutsches Medizinisches Zentrum clinic, a medical skin care center specializing in climatotherapy. The patients completed questionnaires (Skindex-29) to quantify their quality of life at different time points: the day of arrival, the day of departure, and 3 and 6 months after the end of treatment.
Results: Marked improvement in the quality of life scores was measured between the time of arrival to time of departure and to 3 months after the end of treatment.
Conclusions: Dead Sea climatotherapy has a significant positive influence on the quality of life of patients with psoriasis vulgaris and psoriatic arthritis.
Key Words: climatotherapy, Dead Sea, psoriasis, quality of life, Skindex-29
Psoriasis vulgaris is a chronic relapsing disease with aprevalence ranging from 0.5 to 4.6% in various populations worldwide [1]. The disease affects not only physical status but also the patient’s overall wellbeing, including the social and emotional aspects of life [2]. Psoriasis is a systemic disease with
considerable disability, comparable to other major chronic illnesses such as cardiovascular disease and diabetes [3]. The PASI (Psoriasis Area and Severity Index) is a common tool for assessing disease severity [4,5], but it does not relate to
** These authors contributed equally to the study†This study was performed in partial fulfillment of the MD thesis requirements of the Hebrew University-Hadassah Medical School, Jerusalem, Israel
the patient’s quality of life. Previous studies have demonstrated the importance of addressing quality of life in psoriasis due to its significant effect on patients’ psychosocial well-being and functional capabilities [6]. In order to quantify the quality of life aspect of chronic diseases such as psoriasis, several quality of life index methods have been constructed in the form of self-reporting questionnaires [7]
Climatotherapy at the Dead Sea is a known therapeutic option for psoriasis [8]. It takes place at the lowest inhabited place on earth at 419 meters below sea level. This low altitude, combined with the constant haze of salts and minerals, allows prolonged sun exposure without absorption of high doses of ultraviolet radiation; therefore, there is a lower risk of photodamage [9]. Additionally, Dead Sea climatotherapy allows for several other therapeutic advantages in patients with psoria- sis: a) bathing in the Dead Sea, which is rich in minerals and salts, may induce an antiproliferative effect on diseased skin cells; b) a prolonged stay (4 weeks or more) in a vacation-like environment, including supervision by a professional multidisciplinary therapeutic team, has a psychological soothing effect;
c) Social networking and support is provided by other patients suffering from the same chronic disease. In this study we aimed to demonstrate and quantify the grade of improvement in the patient’s quality of life measured before and after completion of Dead Sea climatotherapy
PATIENTS AND METHODS
Patients participating in this study came to the Deutsches Medizinisches Zentrum clinic, located in the Lot Spa Hotel, Ein Bokek, at the Dead Sea, between March and November 2005. They were sent by their health insurance fund in Germany following the failure of other treatments or because of good clinical results during previous therapeutic stays. This prospective study included 119 psoriasis patients ofGerman nationality above the age of 18 years. All participants signed individual written informed consent forms. The recruitment of this group of adult German patients, who did not personally pay for the journey or the treatment and were specifically prefunded for Dead Sea climatotherapy, might have reduced various forms of selection bias
Figure 1. The Skindex-29 Dermatology Survey of Quality of Life (English version, SKINDEX-29© MMChren, 1997, All rights reserved)[10-12]
such as the exclusion of patients of lower socioeconomic status or the inclusion of patients who came for recreational purposes only. The DMZ clinic, situated at the Dead Sea, is a medical dermatology center specialized in climatotherapy for psoriasis and other skin diseases, as well as arthritis, and is managed by dermatology specialists and a qualified medical team (http:// www.dmz-medical-spa.com/). Treatment at the DMZ clinic
comprises the following:
• medical evaluation by a dermatologist, including medical history, sociodemographic details, physical examination and follow-up during the course of treatment
• a personalized climatotherapy program that includes gradual increase of exposure to sunlight
• sea bathing for 20 minutes twice a day
• topical treatments including emollients and/or salicylic acid specifically prescribed for each patient according to his/her skin condition
• nurse availability to help with any medical issue that might arise
• a relatively secluded, stress-free hotel and spa environment.
The study protocol, based on the above principles, was designed to provide each patient individually with a calculated therapeutic ultraviolet B radiation dose plan, while taking into consideration the patient’s skin phototype and the minimal erythema dose, which correlates with the patient’s sensitivity
to ultraviolet radiation. The patients’ parameters of quality of life were evaluated using the Skindex-29 dermatology survey [Figure 1]. This questionnaire was specifically designed to assess quality of life in patients with dermatological conditions. The Skindex-29 was previously tested and validated [10,11] and its German language version, used in the current study, was also previously validated [12]. Permission to use the Skindex-29 in this study was obtained by E.K. from the original Skindex-29 author
(Chren Mary-Margaret MD, personal communication, 2004) and the author of the German version (Augustin Matthias MD, personal communication, 2004). Each question in the survey had a 5 point answer scale, ranging between “never” (0) and “all the time” (5); the lower the score (range 0–100) the better the patient’s overall quality of life . The overall quality of life score can be further divided into three subscales: the patient’s emotional state, symptom severity, and functioning state. Unlike the PASI 2 score, the survey does not quantify physical symptoms but assesses the quality of life impact on the symptom severity subscale. Patients completed the questionnaires at four follow-up time points: upon arrival, at the end of treatment (departure day), and 3 and 6 months after the end of treatment. The questionnaires on the arrival and departure days were completed at the DMZ clinic and the last two were completed in the patients’ homes in Germany and were returned by post. The severity of disease was assessed on arrival at the DMZ clinic by a dermatologist. The assessment was based on the previous treatment received at home and on the disease’s skin involvement. The PASI was recorded only if the lesions covered more than 10% of the body surface area. PASI values were also obtained by the same dermatologist at the end of the treatment.
statistical analysis
Statistical analysis was performed using the paired t-test to evaluate quality of life scores before and after treatment and the ANOVA test for assessing the linear trend over the course of the follow-up. The Greenhouse-Geisser method was applied to calculate the P value for trend. All P value calculations were
two-sided and considered statistically significant if < 0.05. Statistical analyses were performed using SPSS version 15.0 software (Chicago, IL, USA).
Results
The main baseline characteristics of the patients are summarized in Table 1. A total of 119 patients arrived at the DMZ clinic for climatotherapy. Their mean age was 46.8 years; 71% of the patients were males; 61% suffered from psoriasis vulgaris (without any joint involvement) and 39% from psoriatic arthritis. Mean duration of treatment was 4.1 weeks. At the beginning of treatment (arrival day), 71 patients (60%) completed the questionnaires. The response rate gradually decreased at further follow-up points, namely the departure day and 3 and 6 months later [Table 2]. The overall Skindex-29 score decreased, indicating quality of life improvement, by a mean value of 22.8 points (P < 0.001) between arrival and departure times. Quality of life improvement was also measured between the overall mean score at arrival day and the mean scores obtained 3 and 6 months after the end of treatment (-9.2 points, P = 0.008 and -5.2 points, P
Table 1. Baseline characteristics of the 119 study patients with psoriasis
| Mean ± SD | n | % | ||
| Age (yrs) | 46.8 ± 10.6 | 119 | 100 | |
| Male gender | – | 85 | 71 | |
| Type of disease | ||||
| – | 73 | 61 | ||
| Psoriasis | ||||
| Psoriatic arthritis | – | 46 | 39 | |
| Treatment duration (weeks) | 4.1 ± 0.8 | 119 | 100 | |
| Body mass index | 28.3 ± 5.8 | 119 | 100 | |
| PASI* | 13.7 ± 6.5 | 39 | 33 | |
| Overall quality of life score | 49.6 ± 15.9 | 71 | 60 |
PASI = Psoriasis Area and Severity Index
Table 2. Overall quality of life score at different follow-up time points
| Arrival day (n=71) | Departure day (n=70) | 3 months after departure (n=35) | 6 months after departure (n=23) | |
| Overall score ± SD | 49.6 ± 15.9 | 27.6 ± 19.4 | 38.8 ± 19.1 | 43.7 ± 22.2 |
| Improvement from arrival day (%)* | – | -22.8 (45) | -9.2 (20) | -5.2 (11) |
| P value | – | < 0.001 | 0.008 | 0.28 |
= 0.28, not significant, respectively; P for trend = 0.004) [Table2]. Similarly, the quality of life score differences between arrival and departure times and between arrival and the 3 month follow-up point were statistically significant for the emotional, symptom, and functional scores (data not shown).
The linear trend of change in quality of life over the entire study period, between arrival time and 6 months after departure, was significant for the overall quality of life score as well as for the three subscales [Figure 2]. Patients who were over 40 years old had significantly lower mean quality of life improvement than younger patients, ≤ 40 years of age, in the emotional scale (-18.5 ± 21.7 points
vs. -36.0 ± 25.3 points, P = 0.01) and in the functioning scale (-15.1 ± 20.5 points vs. -27.7 ± 20.6 points, P = 0.03) between arrival and departure times. Patients who were obese (body mass index ≥ 30 kg/m2) had significantly lower mean quality of life improvement than non-obese patients in the emotional
scale (-16.3 ± 21.2 points vs. -28.4 ± 24.8 points, P = 0.04) between arrival and departure times.
Mean PASI percent improvement, calculated as the difference between arrival and departure values divided by arrival value, reached 96.8%. The mean overall quality of life and PASI scores at departure time (27.6 ± 19.4 and 0.44 ± 0.77, respectively) had a Pearson correlation coefficient r of 0.27 (n = 26 pairs, P = 0.19).
Figure 2. Skindex-29 questionnaire scores of the overall, emotional, symptoms and functioning quality of life scales at the study follow uptime points*
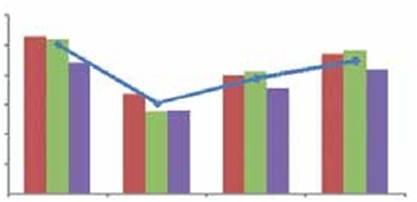
No statistically significant difference in trends over the study period was observed between the overall quality of life score, as well as between the three subscale scores, of patients with psoriasis vulgaris and the corresponding scores of patients with psoriatic arthritis (data not shown).
Discussion
Climatotherapy for psoriasis was established in recent years as a beneficial therapy that improves patients’ physical condition [13,14]; it is also known to be beneficial for various other chronic illnesses such as those of rheumatic [15,16] and cardiovascular origin [17,18]. However, little has been documented on the aspect of patients’ quality of life with regard to climatotherapy. In our study, an improvement in the quality of life of patients with psoriasis vulgaris and psoriatic arthritis who underwent climatotherapy at the DMZ clinic was observed. A statistically significant improvement in the overall quality of life score was observed from the day of arrival to the day of departure and further to 3 months after the end of
treatment by 45% and 20% respectively. These results represent a marked improvement in the quality of life of the participating patients. The quality of life scores obtained 6 months after the end of treatment demonstrated a slight improvement as well. However, this improvement was not statistically significant,
possibly due to the lower number of completed questionnaires at this time point. Notably, two subgroups of patients had lower rates of quality of life improvement, particularly regarding the emotional
aspect of quality of life. These patients were older than 40 or were obese. These patients could therefore benefit from lifestyle modification programs such as weight reduction intervention during the therapeutic stay at the Dead Sea in addition to the existing medical and climatotherapy interventions. A significant improvement in the quality of life in parallel with a marked improvement in the physical skin condition was reported in our study as well as in others [14]. This composite improvement may pose a challenge for measuring the direct contribution of climatotherapy to quality of life versus that of medical treatment alone. In fact, a non-physical outcome of psoriasis, such as its effect on quality of life or depression [19], along with the difficulty to assess the ability of a given therapy to modulate these outcomes directly, can play a major role in the management and prognosis of any chronic morbidity. Further studies may be required to better understand the mechanisms involved in the complex and prolonged interactions between such interventions and outcomes. This concept in psoriasis was recently defined as cumulative life-course impairment [20]. Our report and the accumulating medical research evidence could encourage patients and physicians to consider Dead Sea climatotherapy as a routine therapeutic option for psoriasis. Studies with longer follow-ups and larger sample size could further determine the magnitude of various long-term effects of climatotherapy at the Dead Sea on the quality of life.
Acknowledgment
We thank Ms. Sabine Gelerstain for her administrative support.
corresponding author: dr. e. Kopel Dept. of Dermatology, Hadassah university Hospital, P.O Box 12000,
Jerusalem 91120, Israel
Phone: (972-2) 676-4656,
Fax: (972-2) 676-9036,
email: eran.kopel@mail.huji.ac.il